Autonomic Dysreflexia
What you need to know
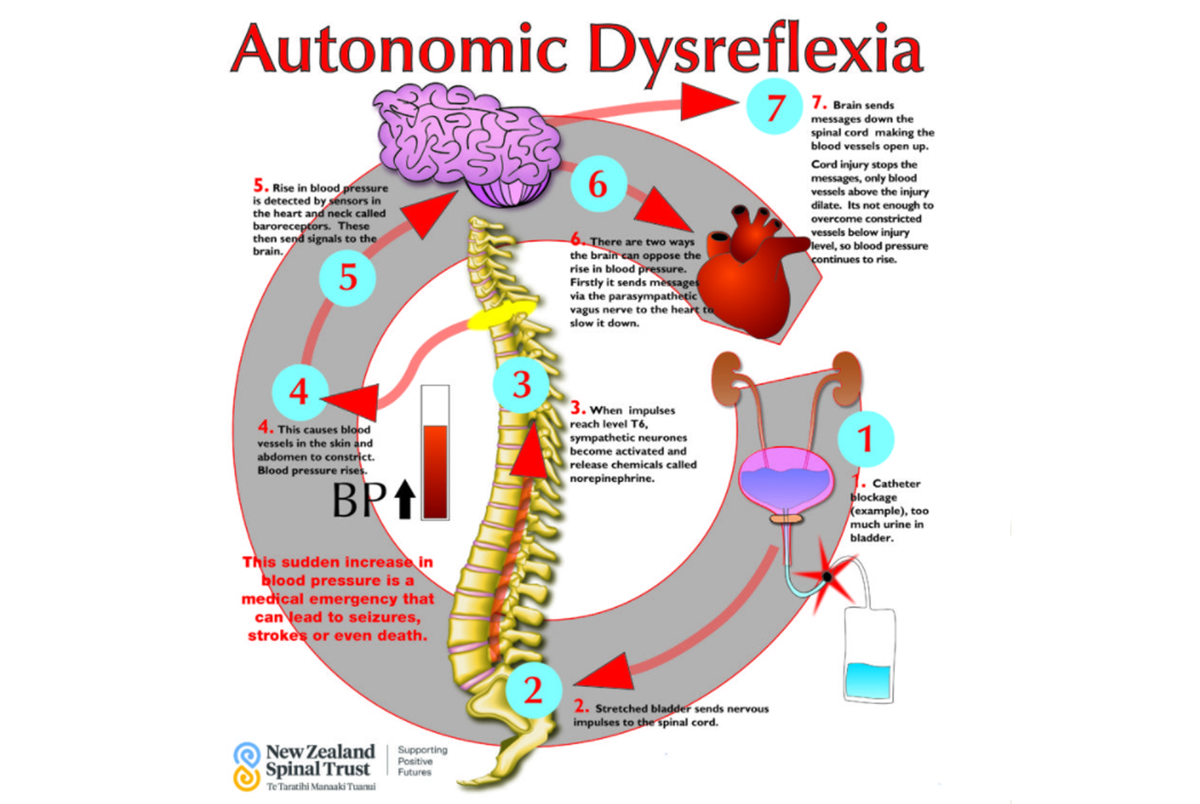
What is Autonomic Dysreflexia?
Autonomic Dysreflexia (AD) is a potentially life-threatening medical emergency that affects people with spinal cord injuries at the T6 level or higher. There have been incidences of some people with T7 and T8 injuries who can develop AD. AD produces a sudden increase in blood pressure requiring immediate emergency attention as inaction can lead to seizures and strokes etc.
For most people, AD can be easily treated as well as prevented. The key is knowing your baseline blood pressure, triggers, and symptoms.
When triggered, AD requires quick and correct action. Because many NZ health professionals are not familiar with this condition, it is important for people who are at risk for AD, including the people close to them, to recognize the symptoms and know how to act.
Signs & Symptoms
- Flushing and sweating above the injury level
- Nasal stuffiness
- Goose bumps and paleness below injury level
- Sudden high blood pressure (hypertension)
- Pounding headache
- Slow heart rate (bradycardia)
- Blurred vision or spots in vision
- Irregular heartbeat
- Anxiety or apprehension
- May have no symptoms (this is known as silent autonomic dysreflexia)
Most Likely Causes
The most common cause for autonomic dysreflexia (AD) is bladder distention or swelling (e.g., due to a blocked catheter or detrusor sphincter dyssynergia), followed by bowel distension.
Other causes:
Bladder or kidney stones, urinary infection, bowel impaction, fracture, heterotopic bone, substance surgery. Pressure area, sunburn, ingrown toenail.
Reproductive – sex, ejaculation, menstruation, pregnancy/labour.
Treatment
- Recognise the signs and symptoms of AD
- Check blood pressure and monitor frequently (NB Patients with SCI above T6 have low systolic blood pressure of 90-110mmHg)
- Sit the person up, lower the legs
- Loosen any clothing or constrictive devices
- Keep an eye on the person and look for the underlying cause and correct if found.
Bladder
- Insert a catheter – if the person does not have one, use lignocaine jelly
- Check existing catheters for kinks, folds, obstructions and correct placement
- If catheter is blocked, irrigate the bladder with 10-15ml saline
- If catheter is not draining, remove and replace it
- If systolic blood pressure (top reading) is raised above 150mmHg, consider giving medication to lower it e.g. Glyceryl Trinitrate (GTN) spray, and pain relief e.g. morphine
- NB if the patient has been on PDE5 Inhibitors (Viagra, Cialis, Levitra) in the last 24 hours, instead of GTN give Nifedipine 10mg sublingual or a crushed tablet under the tongue
- Continue looking for a cause
Bowel
If there is faecal impaction insert lignocaine gel, wait 2 minutes, then insert a lubricated gloved finger into rectum to remove stool
- Look for other causes of AD
- Monitor blood pressure for at least two hours after episode has resolved
- Document episode in medical records
- Review precipitating cause to look for preventative strategies
How can I prevent AD?
Avoid the following triggers:
- Ensure bladder and bowel regimes are followed carefully with adequate bladder drainage
- Keep your catheter free from kinks, keep bag empty and check for grit that may form
- If prone to AD use local anaesthesia before evacuating the bowel
- Have a good skin care routine to avoid pressure areas
- Avoid getting sunburnt
- Eat a well balanced diet with adequate food intake
- Carry an AD card especially if you have to go into hospital or visit a medical centre.
- Educate your family/whānau, friends, carers, doctors etc about AD.
